BSG Clinical Services Excellence Award 2026 2nd place submission by Prof Dhiraj Tripathi, Consultant Hepatologist and Liver Transplant Physician.
Acknowledgements: Dr Cathal Clifford, Dr Ho Tuan Tiong, Dr Helen O'Donovan, Dr Francesca D'Arcangelo, Miss Ellena Taylor, Mrs Kimberley Sayani, Mrs Kiran Chumber, Ms Georgia Salter, Ms Amanda Smith, Sister Maria Round, Dr Debashis Haldar, Mr Russell Bolton, and Dr Neil Rajoriya.
The COVID-19 pandemic significantly affected UK clinical services, resulting in more than 7 million patients on NHS waiting lists for diagnostic and therapeutic services. Endoscopy was adversely affected by its invasive, aerosol-generating nature, leading to significant capacity constraints.
Significant changes faced in our institution post-pandemic included:
- A backlog of patients waiting for variceal surveillance and varices therapy. The waiting list continued to increase despite regular vetting, with more than 1,500 patients awaiting a variceal-related endoscopy by the end of 2024.
- Serious adverse incidents which resulted from patients suffering variceal bleeding while waiting for an endoscopy.
- A sub-optimal endoscopy bookings service, which, despite the best efforts of managers, was affected by a high level of staff turnover. High staff turnover negatively impacted efficiency, timeliness of bookings, and a lack of optimisation of liver slots on designated liver lists (i.e. 2ww GI scopes booked into liver slots)
- Patients being referred for diagnostic endoscopy without due attention to guidance on the use of non-invasive tests (NITs) as advised in the Baveno 6 criteria (doi: 10.1016/j.jhep.2015.05.022) (liver stiffness measurement (LSM) using vibration-controlled transient elastography (VCTE) and platelet count) to select patients for surveillance endoscopy or to commence on non-selective beta-blockers (NSBB) in compensated advanced chronic liver disease (cACLD) and clinically significant portal hypertension (CSPH) as per NICE cirrhosis guidance (https://www.nice.org.uk/guidance/ng50). Thus, many patients did not require endoscopy when they could have been monitored with NITs or initiated on NSBB.
A quality improvement project (QiP) to address the issues outlined above was performed. Fundamental to the QiP was the implementation of current clinical practice guidelines, and engagement from endoscopy administration and managers. We involved a multidisciplinary team to address the challenges.
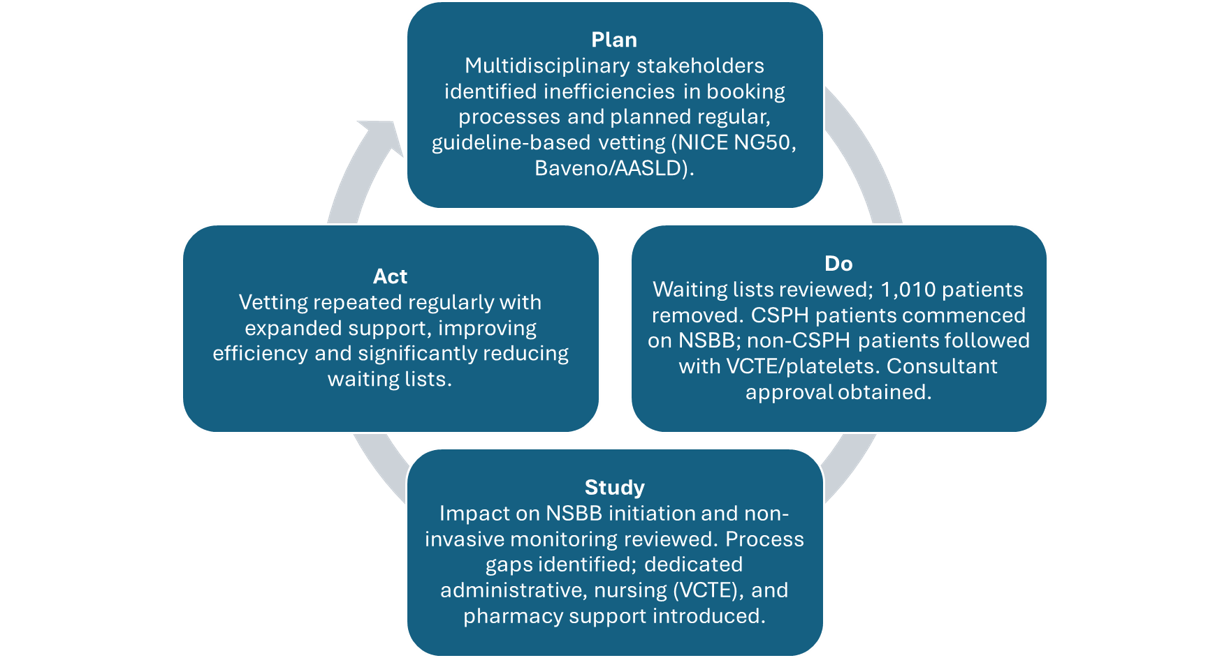
For the QiP, the Model for Improvement was implemented. The aim was to reduce variceal surveillance waiting lists over a 1-year period (Jan 2025-Jan 2026). The Plan-Do-Study-Act (PDSA) method was used, drawing on knowledge gained from a member of the study team (DT) who participated in the BSG Leadership Improvement Programme as part of Project 90. (Figure 1).
Plan: A stakeholder group was convened, including clinicians, managers, and administrative staff. We attempted to address deficiencies in the current booking process and ensure that lists were used efficiently and aligned with the clinical practice guidelines, as mentioned earlier. Regular vetting of requests was planned, with the outcomes monitored closely and the process further refined as necessary.
Do: Data were collected from the variceal surveillance waiting lists, and it was determined that 1,010 patients did not require placement on a liver list. Patients with cACLD and CSPH who could be started on NSBB to prevent decompensation, in accordance with NICE Guidance on Cirrhosis (NG50), were removed from the waiting list. We removed patients with cACLD who did not meet criteria for CSPH but could be followed non-invasively with VCTE and platelet count using Baveno 7 (https://doi.org/10.1016/j.jhep.2021.12.022) /AASLD criteria (DOI: 10.1097/HEP.0000000000000647) to diagnose CSPH. The consultants for all patients proposed for removal from the waiting list, along with the reasons for the proposal, were notified to seek their approval. The medical team conducted rigorous vetting, and the impact of the vetting rules on the initiation of NSBB and non-invasive monitoring was reviewed. The favourable first round of vetting led to a second round under the same rules.
Study: The medical team conducted rigorous vetting, and the impact of the vetting rules on NSBB initiation and non-invasive monitoring was reviewed. Through several meetings with key stakeholders, further insights were gained, using the “lens of profound knowledge,” into the processes that were ineffective for booking vetted patients. Dedicated staff were assigned to manage the liver lists, which ultimately reduced the waiting list. Further support was provided by nursing (clinics for VCTE) and allied health staff (Band 8 pharmacist for initiating and monitoring non-selective beta-blockers (NSBB)).
Act: The favourable first round of vetting led to a second round under the same rules, with additional support from administrative staff, nursing and pharmacy. This led to a significant reduction in the waiting list due to improved efficiency. Vetting was conducted regularly and monitored.
Figure 1: PDSA Cycle for Optimising Variceal Surveillance Lists
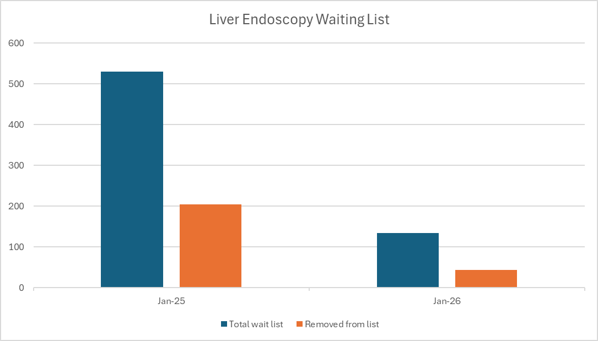
The waiting list for liver endoscopy at the start of the QiP in January 2025 was 530 patients. Vetting was done on this list of patients. Ninety eight (18.5%) patients were removed from the waiting list because they could be started on NSBB; 57 (10.8%) did not require endoscopy for other reasons; and 49 (9.2%) were followed up with non-invasive tests.
During a further round of vetting at the end of 2025, the waiting list of 134 patients was significantly reduced. Of these patients, 44 (32.8%) could be removed and started on NSBB, or monitored using non-invasive tests (see Figure 2).
Overall, the QiP removed 248 patients from the waiting list, resulting in a 74% reduction in the waiting list, creating capacity for new slots for high-priority patients, e.g., those on a variceal banding programme.
The pharmacy-led service has so far been referred 108 patients, initially identified through the QIP vetting process, and, more recently, patients have also been prospectively referred. Initial screening identified 36 (33.3%) patients as unsuitable for NSBB due to medical contraindications, prior intolerance, or patient or clinician preference, among other reasons. To date, among the 47 (43.5%) patients started on carvedilol, more than 80% have been titrated to the optimal dose (12.5mg/24 hours), with the remainder undergoing further titration. Self-reported adherence has been very good.
There are also potential cost savings, as a 28-day course of carvedilol 6.25mg bd costs £2.06, compared with the HRG cost of a diagnostic upper GI endoscopy at £710. Since 248 patients were removed from the waiting list, the cost savings from avoided endoscopies are at least £176,000. The cost of initiating carvedilol in 47 patients per month is £96.10.
Figure 2: Impact of QiP on liver endoscopy waiting list
The key learning points:
- Demonstrate the clear need for change with examples. We identified the inefficiencies in the processes using the “lens of profound knowledge” approach. A formal presentation to the speciality highlighted the areas requiring change.
- Stakeholder involvement: A key reason for the lack of progress prior to the QiP was inconsistent stakeholder engagement. We spent considerable time and effort convening a representative stakeholder group capable of influencing change and culture. We reached a unanimous decision to improve the current situation and change the approach.
- Methodology: The Model for Improvement and PDSA cycles were developed. We applied the principles rigorously, making PDSA the standard approach.
- Support from multidisciplinary clinical team: We were very clear with the key stakeholders of the aims and goals, and their involvement. This greatly helped engagement during the QiP, e.g. support for consultants, pharmacy, and nursing.
- Embed change and ensure fidelity of the processes: We ensured that there was a continuous improvement through regular meetings with the key stakeholders. Additional audit cycles are planned to ensure continued process fidelity.