BSG Clinical Services Excellence Award 2026 highly commended submission by Dr Carolin Henson, Consultant Gastroenterologist.
What were the challenges and why did the service need to change?
30,000 patients per year have pelvic radiotherapy in the UK. Survival is improving, meaning more people are living long enough to develop side effects. One of the most common side effects is radiation proctopathy (RP), which causes severe bleeding in 6% patients.
There are few effective, safe, evidence-based treatments for RP, often leading to patients passing repeatedly through the HSC pathways receiving suboptimal, often ineffective treatments.
One of the few specialist services for RP is based at Wythenshawe Hospital, Manchester. This is a supra-regional service, which serves predominantly Greater Manchester, Cheshire, Lancashire and Merseyside. This service provided sucralfate enemas and Purastat, but could not provide radiofrequency ablation (RFA), despite it being shown to be safe and effective1, due to lack of access to an RFA generator. Several hospitals in the area provided RFA but not for RP. This exposed a gap in service and an area of unmet clinical need.
How did you overcome the challenge?
The endoscopist expertise was available at Wythenshawe Hospital to deliver RFA. Referral pathways from oncology and surgery were well-established. The main barrier to provision of the service was access to the RFA generator (Medtronic). Nurse training was also required.
A short-term solution was implemented, whereby patients with refractory RP were treated with RFA in Liverpool. Initially local Trusts providing a Barrett’s oesophagus RFA service were approached to provide RFA for RP or lists for the generator to be used to treat RP. Unfortunately there was no capacity.
A fully-costed business case to procure the RFA generator at Wythenshawe Hospital to treat RP was submitted and approved. The board stated this was the most clinically compelling case they had reviewed. Unfortunately, in March 2020, the Covid-19 pandemic upended healthcare systems worldwide. Approved business cases were initially put on hold, then revoked. This was a devastating blow to our patients and our service.
Fortunately, in 2022, a generous personal donation from a relatives’ family enabled the procurement of the much-needed generator. No training was required for the endoscopist, but a rolling programme of training for the nursing staff commenced in Summer 2023. We started treating patients in October 2023.
What were the outcomes?
Since October 2023, 17 patients with haemorrhagic RP have been treated with RFA in a mean number of 1.6 (1-2) sessions. Initially RFA was offered to those with refractory bleeding after Purastat +/- sucralfate enemas. We now offer RFA as first line treatment, especially for patients with severe, transfusion-dependent bleeding and those requiring anticoagulation/antiplatelets.
RFA is delivered on a 12-weekly basis, with a telephone consultation 8 weeks after each treatment to determine if further RFA is required. Oral bowel preparation is used. RFA is delivered using a through-the-scope device and a 2 hits no clean technique.
Table 1 shows baseline demographic and clinical data. All patients reported at least weekly bleeding and 5 were incontinent of blood.
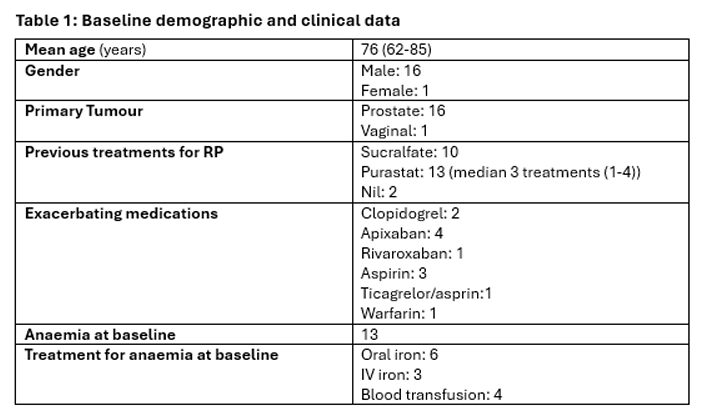
Healthcare utilisation in this group of patients pre-RFA was high. Patients had a median of 1 (0-3) lower GI endoscopies before referral and a median of 3 (0-7) lower GI endoscopies following referral before RFA, often due to Purastat delivery.
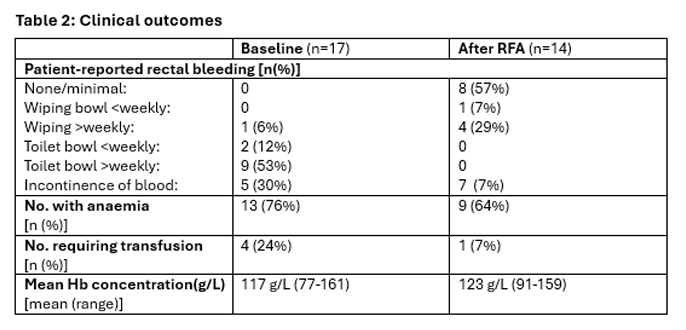
Clinical outcomes are shown in Table 2. Within 1-2 treatments bleeding was reduced to minimal levels in two thirds of patients, with third reducing to blood on wiping only. This appears to be better than the published outcomes for Purastat, which halves the number of rectal bleeding episodes in a median of 3 treatments2.
Alongside this, transfusion-requirement reduced. All transfusion-dependent patients prior to treatment did not require transfusion afterwards, except one.
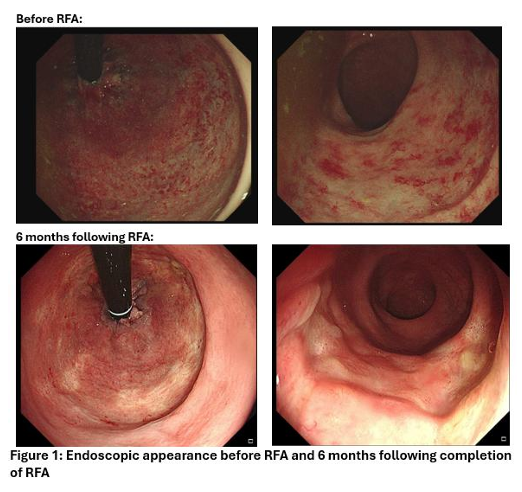
Median rectal telangiectasia density score, improved from grade 3 to grade 2 (Figure 1). Importantly, 7/12 (58%) patients restarted anticoagulation/antiplatelets after RFA, thereby reducing cardiovascular risk.
RFA is safe, with few adverse events: spontaneously-resolving early bleeding(3);asymptomatic superficial ulceration(2). One had refractory transfusion dependent bleeding requiring defunctioning colostomy. He did not tolerate bowel preparation so only had 1 RFA session.
Patient experience is excellent, improving quality-of-life through bleeding control, with one previously transfusion-dependent patient describing the results as “transformative”.
What were the learning points and how can this influence other teams?
To the best of our knowledge, this is the first dedicated RFA service for RP. Our service has demonstrated the successful integration of RFA into a unit where it had previously been unavailable, and the significant benefit to patients. A simple training process for nurses was effective and, in future, new endoscopists will undergo training.
One of the criticisms of RFA is cost, but this must be balanced with the impact of inadequately treated disease on healthcare cost and symptom burden.
The implementation of this service corroborates the safety of RFA for RP and benefits in terms of both rectal bleeding reduction; endoscopic obliteration of the angioectasia; and ability to recommence anticoagulation/antiplatelets. The latter has the secondary benefit of reduction in cardiovascular risk, which is critical for this demographic and has the potential to further reduce healthcare utilisation and associated costs.
There is minimal expense in setting up a service, especially if an RFA generator is already available. Improving access to RFA for RP has the potential to reduce healthcare utilisation and costs, especially if used in appropriate patients first-line. This reduction in utilisation will also reduce demands and increase much-needed capacity in our overstretched endoscopy units. RFA successfully minimises bleeding and significantly improved endoscopic appearance in 1-2 treatments, which offsets the costs when compared to less effective, but seemingly cheaper treatments.
We would encourage developing a national network of providers of RFA for RP to improve access and obtain good quality outcome data, to the benefit of patients and healthcare services.
References
- McCarty TR, Garg R, Rustagi T. Efficacy and safety of radiofrequency ablation for treatment of chronic radiation proctitis: A systematic review and meta-analysis. Journal of Gastroenterology and Hepatology. 2019;34(9):1479-1485.
- White K, Henson C. Endoscopically-delivered Purastat for the treatment of severe haemorrhagic radiation proctopathy: a case series. GUT. 2019;68 (Suppl 2):A195-A196.