BSG Clinical Services Excellence Award 2026 1st place submission by Dr Rebecca Smith, IBD Research Fellow.
Acknowledgements: Rebecca Smith, Vida Cairnes, Sarah Hawkins, Halina Daniels, Nina Winter, Clare Redstone, Sally Payton, Michelle Clarke, Sandra Smith, Laura Dickinson, Lucy Moore, Suzi Marriot, Andrew Davis, Richard Appleby, Judyta Lomza, Monica Chan, Cherie Fothergill, Jackie Scarse, John Rogers, Jonathan Digby-Bell, Tarek Shirazi, Shyam Prasad, Chris Calvert, Jennie Clough, Phoebe Hodges, Sean Mole, Nathan Kuk, Safwat Odeh, Chris Roberts, Rebecca Smith, Maria Bishara, Fakhirah Badrulhisham, Desmond Chee, Malik Janjua, Simeng Lin, Neil Chanchlani, Neel Heerasing, Amanda Laing, Gareth Walker, Graham Heape, Ben Hamilton, Keith Pohl, Claire Gordon, Peter Hendy, Claire Bewshea, Yousra Djouider, Daisy Pamment, Nick Kennedy, James Goodhand, and Tariq Ahmad.
What were the challenges and why did the service need to change?
Timely diagnosis and treatment of inflammatory bowel disease (IBD) is important because earlier disease control reduces disease-related complications1. Diagnostic delay is also associated with a reduced quality of life2 and workplace productivity3 and increased healthcare usage4. There is considerable interest, therefore, in strategies that reduce the time-to-diagnosis of IBD.
In the United Kingdom, general practitioners refer patients with symptoms suggestive of IBD to colorectal surgeons, gastroenterologists, emergency department physicians or directly for lower gastrointestinal endoscopy.
Since the early adoption of stool calprotectin testing in primary care in 20105 we have aimed to reduce the time-to-diagnosis and treatment of IBD using iterative Plan-Do-Study-Act (PDSA) cycles (Figure 1.)
PDSA cycle 1: Quality improvement project to identify factors associated with a delay in IBD diagnosis (ref)
Between 2014 and 2017, we undertook a prospective quality improvement study across 49 primary care practices to define the time-to-IBD diagnosis6. We showed that the longest component of the time-to-diagnosis was patient-related delay; that using a calprotectin-led referral pathway led to minimal primary care delay; but that there was significant variability in the time to diagnosis and treatment in secondary care6.
Mapping of our secondary care pathway identified multiple steps between referral and treatment. Consequently, responsibility passed between teams and delays occurred between endoscopy, clinical review and before treatment initiation.
PDSA cycle 2: Automated electronic case finding of patients with newly diagnosed IBD and triage to specialist IBD clinic
In 2018, we created an electronic algorithm that screened all endoscopy and histology reports for patients with a new diagnosis of IBD who were then allocated to a specialist IBD clinic7. In parallel, our IBD nursing team provided training to our non-medical endoscopists to enable same-day treatment initiation.
These measures led to a modest reduction in the median time from referral to first treatment and specialist clinic review and were associated with an increase in the proportion of patients receiving an advanced therapy in the first year after diagnosis (Figure 1). However, marked variability in referral triage practices of patients with suspected IBD was observed.
PDSA cycle 3: Referral triage of patients with ‘suspected IBD’ to weekly dedicated IBD clinics
From 2024, patients referred with symptoms and/or biochemical markers suggestive of IBD were triaged to a new dedicated suspected IBD clinic and typically offered an appointment within one week.
This created a single-structured route for patients with suspected IBD with ring-fenced endoscopy appointments scheduled at the time of clinic review with early access to research. We continued to use our automated electronic case finding algorithm to identify patients diagnosed on other pathways
Collectively these measures halved the median time from referral to first treatment, specialist clinic review, emergency presentations, readmissions and surgeries in the first year.
PDSA cycle 4: Direct to public calprotectin and FIT testing
Why some people wait so long to present with gastrointestinal symptoms is unclear. Recent reports in patients with sexually transmitted infections and hepatitis C, where stigma and embarrassment are common, suggest that this barrier may be overcome by the anonymity of direct-to-public testing8,9.
We have shown that in the UK direct-to-public calprotectin testing is already readily available from multiple providers. Consumers can choose between cheap, rapid lateral flow tests or send stool samples for gold-standard laboratory testing but ongoing care pathways in the setting of positive and negative results were limited10.
Between 2024-25, as part of the Redesigning a faster pathway to IBD diagnosis (RAPID) research program, we sought in 200 newly diagnosed patients with IBD the self-reported barriers to presentation (see Word Cloud Figure 2)11. Central themes related to limited access to GP appointments, being missed diagnosed and the apprehension of invasive tests.
What were the learning points and how can this influence other teams?
Patient-related delay is the longest component of the time-to-diagnosis of IBD. Our most recent work suggests this is driven by difficulty accessing GP appointments, missed diagnoses, and the fear of invasive tests. Reducing patient delay is likely to be challenging and novel pathways, such as direct consumer stool testing, need to be tested.
Primary-care delay is minimal using a calprotectin-based referral pathway.
Secondary-care delay can be dramatically reduced using standardised triage for patients with suspected IBD to a rapid access clinic and use of a case-finding electronic tool to identify patients diagnosed on other pathways with ring-fenced endoscopy appointment availability.
All the interventions described use standard hospital systems, electronic reporting and clinic redesign rather than the introduction of bespoke technology. As a result, the pathway components can be implemented within existing service structures and are applicable to other centres seeking to improve timeliness of diagnosis and treatment. The dedicated IBD clinics also provide focused clinical exposure for trainees and specialist nurses, supporting skill development within the multidisciplinary team.
Current PDSA cycle: Redesigning a faster pathway to IBD diagnosis (RAPID) –www.redcap.link/orderatest
In our current work supported by Crohn’s & Colitis UK, the UK NIHR, MAST Ltd, Wetherspoons, local pharmacies and Exeter City Football Club we are evaluating direct-to-public FIT and calprotectin stool testing of 5000 people with symptoms suggestive of IBD. Symptomatic people aged 16-49 years can request a free kit and participants with a positive test are invited to a clinic appointment and colonoscopy as appropriate.
Figures and table text
Figure 1. Iterative quality improvement approach
Sequential Plan–Do–Study–Act cycles used to introduce, evaluate and refine pathway interventions over time.
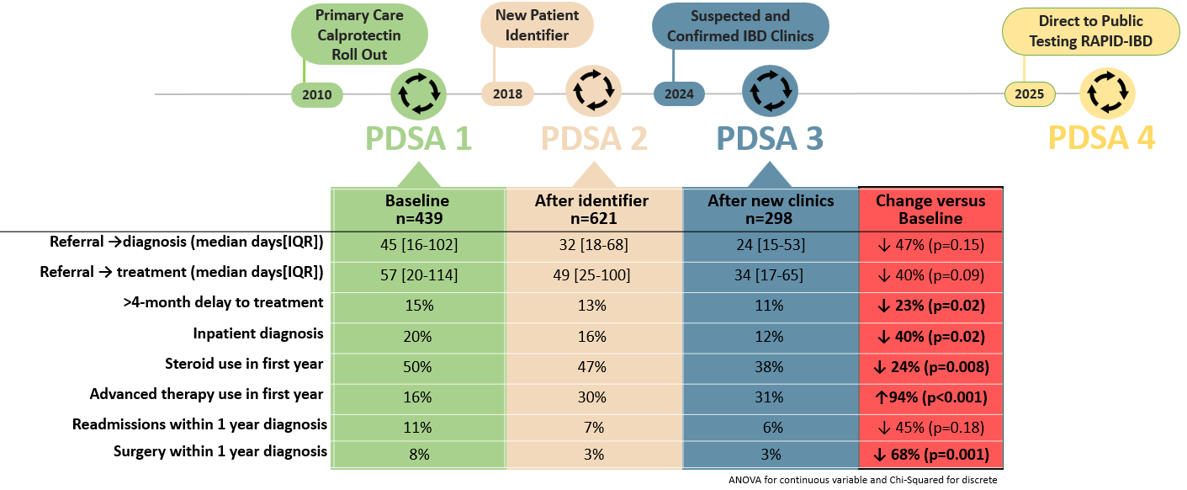
Figure 2. Word Cloud 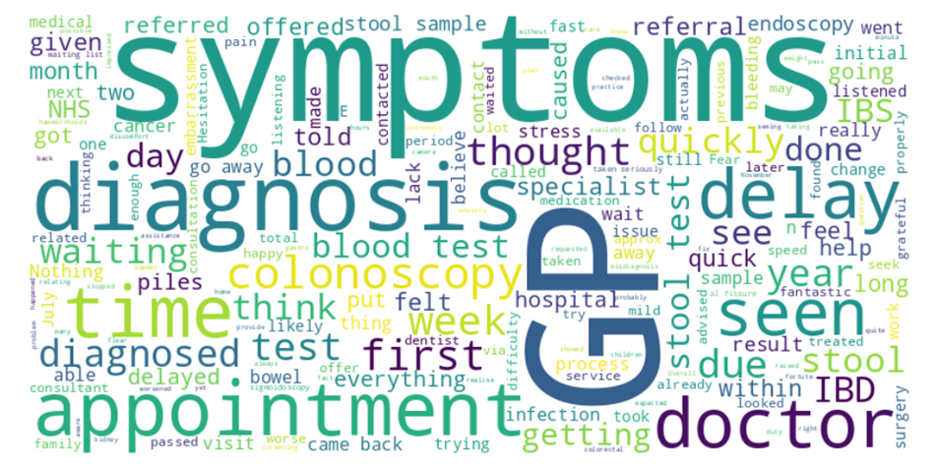
References
- Jayasooriya N, Baillie S, Blackwell J, Bottle A, Petersen I, Creese H, Saxena S, Pollok RC; POP-IBD study group. Systematic review with meta-analysis: Time to diagnosis and the impact of delayed diagnosis on clinical outcomes in inflammatory bowel disease. Aliment Pharmacol Ther. 2023 Mar;57(6):635-652. doi: 10.1111/apt.17370. Epub 2023 Jan 10. PMID: 36627691.
- Souaid C, Fares E, Primard P, Macaigne G, El Hajj W, Nahon S. A review investigating delays in Crohn's disease diagnosis. Clin Res Hepatol Gastroenterol. 2025Jan;49(1):102500. doi: 10.1016/j.clinre.2024.102500. Epub 2024 Nov 15. PMID: 39551466.
- Youssef M, Hossein-Javaheri N, Hoxha T, Mallouk C, Tandon P. Work Productivity Impairment in Persons with Inflammatory Bowel Diseases: A Systematic Review and Meta-analysis. J Crohns Colitis. 2024 Sep 3;18(9):1486-1504. doi: 10.1093/ecco-jcc/jjae057. PMID: 38647194; PMCID: PMC11369077.
- Jayasooriya N, Saxena S, Blackwell J, Bottle A, Creese H, Petersen I, et al. Associations between prior healthcare use, time to diagnosis, and clinical outcomes in inflammatory bowel disease: a nationally representative population-based cohort study. BMJ Open Gastroenterology. 2024;11:e001371. https://doi.org/10.1136/bmjgast-2024-001371
- Walker GJ et al. Primary care faecal calprotectin testing in children with suspected inflammatory bowel disease: a diagnostic accuracy study. Arch Dis Child. 2020 Oct;105(10):957-963.
- Walker GJ, Lin S, Chanchlani N, Thomas A, Hendy P, Heerasing N, Moore L, Green HD, Chee D, Bewshea C, Mays J, Kennedy NA, Ahmad T, Goodhand JR. Quality improvement project identifies factors associated with delay in IBD diagnosis. Aliment Pharmacol Ther. 2020 Aug;52(3):471-480. doi: 10.1111/apt.15885. Epub 2020 Jun 23. PMID: 32573819.
- Chee D, Hamilton B, Cairnes V, et al. P246 Development of a new Inflammatory Bowel Disease Patient Identifier shortens time to clinic review and initiation of treatment. J Crohns Colitis. 2021;15:S288–9. doi: 10.1093/ecco-jcc/jjab076.372
- Gilbert M, Thomson K, Salway T, Haag D, Grennan T, Fairley CK, Buchner C, Krajden M, Kendall P, Shoveller J, Ogilvie G. Differences in experiences of barriers to STI testing between clients of the internet-based diagnostic testing service GetCheckedOnline.com and an STI clinic in Vancouver, Canada. Sex Transm Infect. 2019 Mar;95(2):151-156. https://doi: 10.1136/sextrans-2017-053325.
- Hayes MJ, Beavon E, Traeger MW, Dillon JF, Radley A, Nielsen S, Byrne CJ, Richmond J, Higgs P, Hellard ME, Doyle JS. Viral hepatitis testing and treatment in community pharmacies: a systematic review and meta-analysis. EClinicalMedicine. 2024 Feb 27;69:102489. doi: 10.1016/j.eclinm.2024.102489. PMID: 38440399; PMCID: PMC10909633.
- Bishara M, Smith R, Roberts C, et alCross-sectional evaluation of online direct-to-public calprotectin testingFrontline Gastroenterology 2024;15:352-358
- Smith R, Cairnes V, Bishara M, et al. P0433 Re-designing A faster Pathway to IBD Diagnosis (RAPID-IBD): Phase 1. J Crohns Colitis. 2026;20. doi: 10.1093/ecco-jcc/jjaf231.614