BSG CSSC Service Development Prize 2022 3rd place submission by Dr Paul Brennan.
Hepatitis C virus (HCV) represents a significant global health burden. Approximately 58 million people are estimated to be living with chronic HCV worldwide(1). Chronic infection may lead to several hepatic sequelae including cirrhosis and hepatocellular carcinoma which were primarily responsible for the majority of the 399,000 HCV-related deaths in 2016(2).
The prevalence of HCV in the UK is estimated to have fallen in recent years, from 174,000 in 2015 to 118,000 in 2019(3). The advent of direct acting antiviral (DAA) treatment, with few side effects and a sustained virological response (SVR) above 95%(4), mean that cure can be achieved in the vast majority of HCV cases. There is a realisation that elimination will not be achieved by harm reduction interventions such as needle exchange and opioid agonist therapy alone, so assertive Treatment-as-Prevention strategies need to be assessed for their impact on HCV prevalence(5).
The World Health Organization (WHO) set ambitious targets for the control and elimination of viral hepatitis. For HCV the WHO’s global 2030 elimination targets are 90% of the HCV population diagnosed and 80% successfully treated(6).
These targets have generated much work around implement and delivering on these targets. While national strategies and plans are needed, delivery on the ground will be within communities, areas and regions(7). This has led to the concept of “Micro-elimination” where HCV is eliminated in defined communities or groups, often with specialised interventions(8). However, the scale and balance of these specialised interventions for diagnosis and treatment compared to standard health care environments is unclear.
This project aimed to achieve the WHO HCV diagnosis and treatment targets, using a series of micro-elimination interventions, combined with standard medical care, we evaluated the relative efficacy and contributions of these interventions toward HCV elimination.
Study design
This was a whole population study conducted in a geographically defined region. Within Tayside, HCV services were led and coordinated through a managed care network, which brought together stakeholders and partners from public services and third sector(9).
Data regarding HCV testing was gathered from individuals over 18, previously tested for HCV in National Health Service (NHS) Tayside between January 1999 and June 2020(10).
In 2015 after the development and evaluation of new diagnostic and treatment technology (DBST and DAA treatment respectively), there was a substantial change in the standard of care for HCV. This saw the introduction of multiple interventions for HCV testing and treatment in NHS Tayside with the objective of achieving elimination of HCV as a public health threat(11). Analysis of the characteristics, risk factors and treatment outcomes for individuals tested across all pathways were therefore limited to the years 2015 to 2017 inclusive, to make equal comparisons across the pathways.
The work received Caldicott ethical approval from the NHS Tayside Caldicott Guardian.
Testing
Standard testing for HCV infection uses venous blood for HCV antibodies with subsequent, HCV PCR test of venous blood to confirm active infection. Additionally, dry blood spot testing (DBST) for HCV antibody testing is used in those difficult to achieve venepuncture or in care pathways where venepuncture skills are not available. Follow-up HCV PCR testing can also be performed on DBS. DBST HCV Ab testing was introduced in Tayside in 2009(12). Community pharmacy staff and non-clinical support workers are trained to deliver DBST, enabling task shifting from clinical to community settings(7),(13).
Care pathways
A matrix of five diagnostic pathways were developed to test and treat infected populations in Tayside (Figure 1):
Primary/secondary care: In routine health care settings e.g., general practice/family practice or non-HCV specialist hospital practice, if there is suspicion of HCV infection, an anti-HCV antibody test is requested via standard systems.
Drug treatment services: Individuals recovering from opiate dependence, mostly from injection use, are offered engagement with the Substance Misuse Service and treatment with opiate agonist therapy (OAT). Antibody positive individuals are followed up by a confirmatory HCV PCR as well as baseline blood tests for assessment of liver function and fibrosis assessment The patient is then treated by a HCV specialist nurse embedded in the addiction service, with support from the HCV service multi-disciplinary team.
Community pharmacies: This pathway specifically targets clients in receipt of OAT who are predominantly previous or current people who inject drugs (PWID). They attend pharmacies to pick up OAT regularly, often daily. If the patient tests positive for HCV infection, the case is non-complex (bloods results within set parameters, assessed by the pharmacists as per protocol), and the community pharmacist is an independent prescriber or can use a patient group direction (PGD)(14), the client can be initiated on DAA treatment and monitored by the community pharmacist.
Injecting equipment provision sites (IEPS): In the UK, clean injecting equipment and related paraphernalia are provided to PWID at no cost, from participating community pharmacies and larger dedicated provision sites in collaboration with third-sector partners. People attending IEPS can be offered HCV testing via DBS by trained third-sector workers, or via traditional phlebotomy by NHS staff. If the HCV RNA test is positive, patients are invited to attend a nurse led HCV outreach clinic situated in the IEPS to be started on HCV treatment, which is monitored by HCV specialist nurses with multi-disciplinary team (MDT) support.
Prisons: On entry to prison, new inmates are offered HCV testing. If the test results confirm an individual has active HCV, they are initiated on DAA treatment by a HCV specialist nurse in an in-reach clinic within the prison, supported by the HCV MDT. If an individual is liberated prior to treatment completion, they are provided with the remaining DAA treatment course upon release and followed up in the community to ensure SVR.
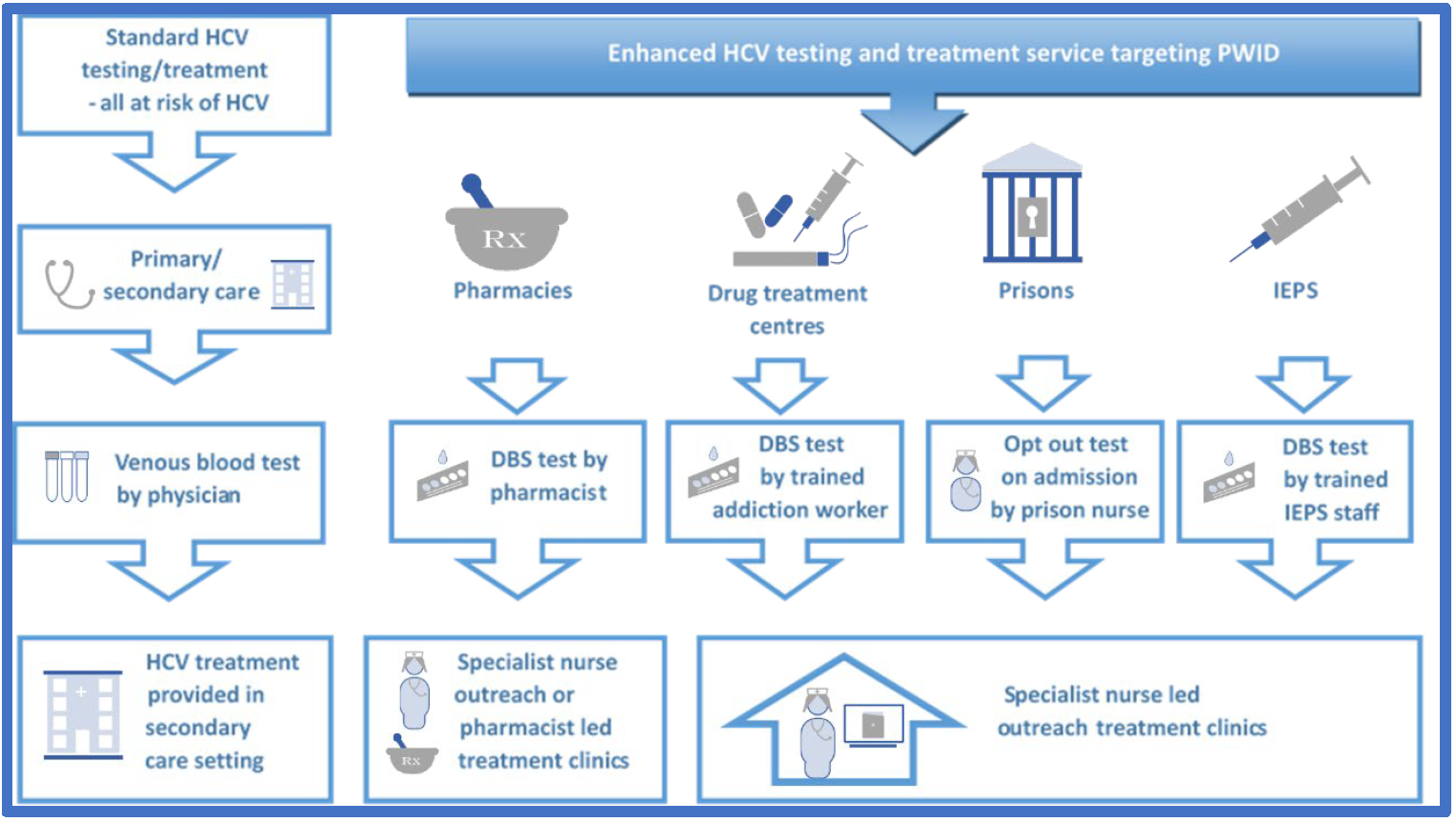 Fig 1: HCV diagnosis and treatment pathways in NHS Tayside
Fig 1: HCV diagnosis and treatment pathways in NHS Tayside
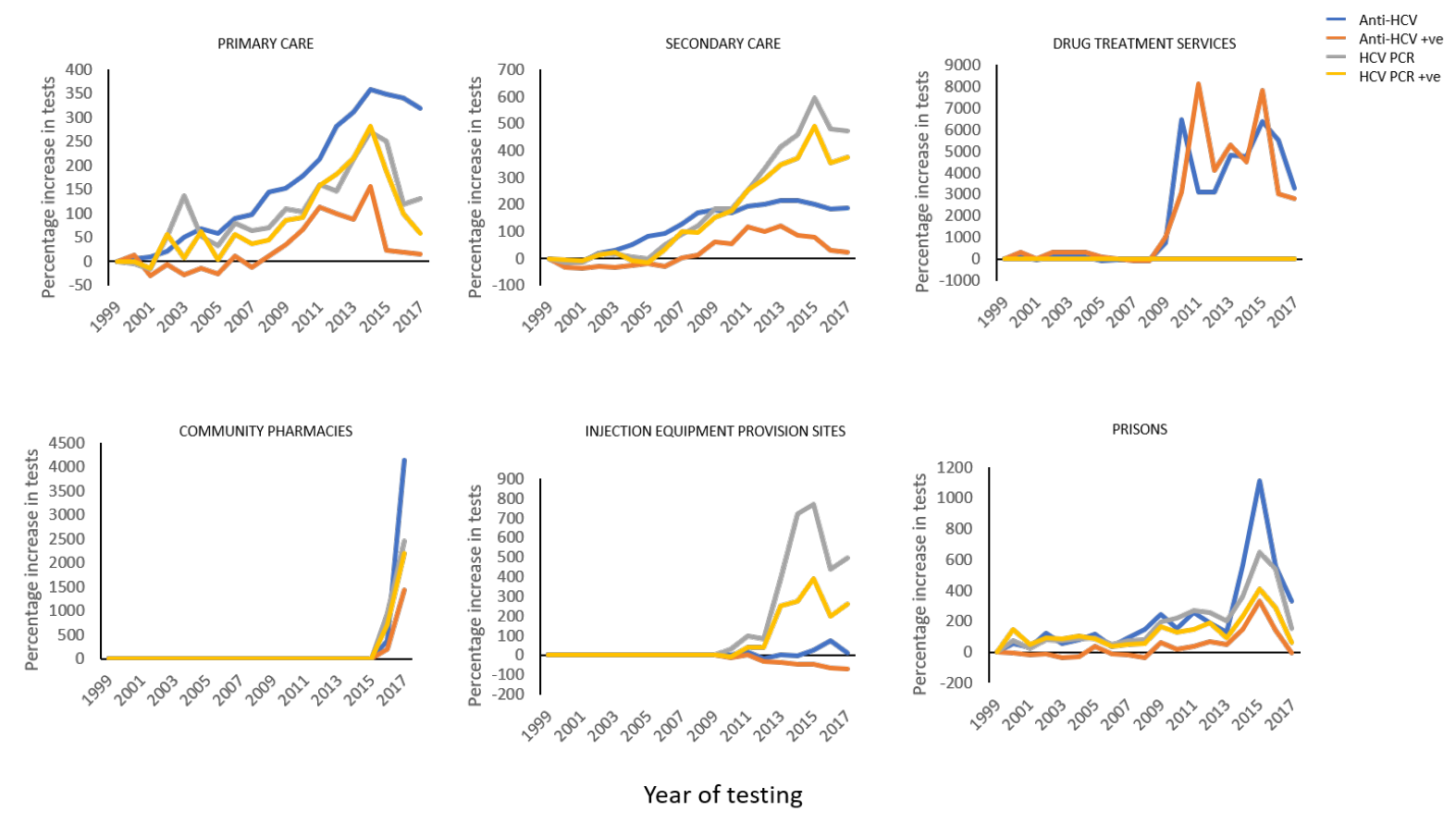 Fig 2: Evolution of testing strategy uptake from 1999-2017
Fig 2: Evolution of testing strategy uptake from 1999-2017
Outcomes
As of June 2020, 94.8% of the estimated prevalence of HCV positive patients in Tayside have been diagnosed and 87.2% have been cured.
From this work it is apparent that all testing pathways engage different cohorts and risk groups of patients, even reaching sub-sections of PWID populations, such as those on OAT. This widespread engagement has been effective in linking patients to treatment across all pathways, bringing the overall prevalence of HCV infection in NHS Tayside steadily downwards.
The recent reduction in PCR positive patients across all pathways in recent years clearly indicates that the pathways employed in Tayside have identified close to all HCV patients in the region. These results provide strong evidence that this matrix of diagnostic pathways was an effective combination to facilitate regional HCV elimination in line with WHO targets.
References
1. Global HIV Hepatitis and Sexually Transmitted Infections Programmes. Global progress report on HIV, viral hepatitis and sexually transmitted infections, 2021. Who 53, (2021).
2. WHO. Hepatitis C. (2020).
3. Public Health England. Hepatitis C in the UK 2020. (2020).
4. Falade-Nwulia, O. et al. Oral direct-acting agent therapy for hepatitis c virus infection: A systematic review. Annals of Internal Medicine 166, 637–648 (2017).
5. Martin, N. K. et al. Hepatitis C virus treatment for prevention among people who inject drugs: Modeling treatment scale-up in the age of direct-acting antivirals. Hepatology 58, 1598–1609 (2013).
6. World Health Organization. Combating hepatitis B and C to reach elimination by 2030: advocacy brief. World Heal. Organ. (2016).
7. Oru, E., Trickey, A., Shirali, R., Kanters, S. & Easterbrook, P. Decentralisation, integration, and task-shifting in hepatitis C virus infection testing and treatment: a global systematic review and meta-analysis. Lancet Glob. Heal. 9, e431–e445 (2021).
8. JV, L., S, W., M, C. & M, T. Micro-elimination - A path to global elimination of hepatitis C. J. Hepatol. 67, 665–666 (2017).
9. JM, T. et al. Multidisciplinary managed care networks-Life-saving interventions for hepatitis C patients. J. Viral Hepat. 24, 207–215 (2017).
10. Mckenzie, P. NHS Tayside Information Governance Caldicott Approval Procedure. (2010).
11. Pedrana, A., Munari, S., Stoové, M., Doyle, J. & Hellard, M. The phases of hepatitis C elimination: achieving WHO elimination targets. Lancet Gastroenterol. Hepatol. 6, 6–8 (2021).
12. JM, T., BP, S., PG, M., M, E. & JF, D. Dry blood spot testing for hepatitis C in people who injected drugs: reaching the populations other tests cannot reach. Frontline Gastroenterol. 4, 255–262 (2013).
13. JF, D. Strategies to foster task-shifting and broaden models of HCV prevention and care. in 7th International Symposium on Hepatitis Care in Substance Users (2018).
14. Medicines and Healthcare products Regulatory Agency. Patient group directions: who can use them. (2017).