BSG CSSC Service Development Prize 2023 highly commended submission by Dr Cheh Kuan Tai
Names of team involved: Mrs Donna Hodge, Lead Upper GI Cancer Clinical Nurse Specialist Miss Eleanor Brothwood, Service Manager for Gastroenterology, Dr Cheh Kuan Tai, Consultant Gastroenterologist, Dr Andreas Koutsoumpas, Consultant Gastroenterologist, Dr Kalpesh Besherdas, Consultant Gastroenterologist.
What were the challenges to your service and why you needed to change?
The first wave of the covid-19 pandemic led to significant changes to our service. Beyond the need to cover the backlog from the loss of elective endoscopy and clinic provision, the way we work changed dramatically. The need to reduce the risk of patients travelling into acute hospitals for outpatient appointments led to dramatic increase in update of telephone or video consultations during the pandemic and post pandemic recovery period. There was also significant development and improvements in our IT infrastructure which led to development of novel digital pathways.
Furthermore, in 2021, the 28 day faster diagnosis standard (FDS) replaced the previous 2WW standard. In this FDS, units are required to communicate within 28 days, cancer diagnosis or rule out in patients who are referred on the cancer pathway.
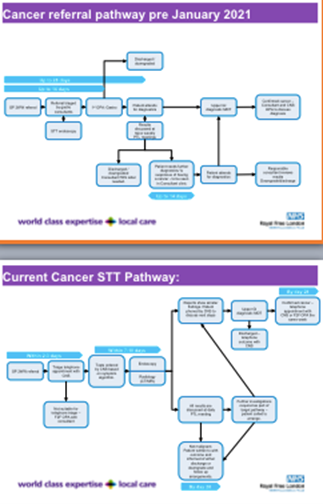
Barnet and Chase Farm Hospitals are district general hospitals which merged in 1999 and serve a catchment area of over 500,000 people. In 2021, we developed a novel nurse-run digital cancer service. The development of this new service involved the development of algorithms for investigations based on symptoms or findings. These algorithms are evidence-based and constantly evolving following our experience in using the pathway. The algorithms were developed in an MDT fashion with involvement of radiologists, gastroenterologists, hepatologists and clinical nurse specialist (CNS). The algorithms ensure targeted systems review questions are answered and the appropriate tests are requested.
How did you overcome the challenges?
The service is led by a gastroenterologist and CNS and also involves 2 other cancer pathway navigators, 1 pathway manager, 1 service manager, 2.6 WTE UGI CNS and 8 other gastroenterology consultants.
Where patients are being discharged with a benign diagnosis which does not require follow-up such as hiatus hernia, all patients are sent patient information and advice. In cases where follow-up endoscopy is required such as in Barrett’s oesophagus, patients are also sent information on this and follow-up endoscopy are booked.
What were the outcomes?
In our first year, between April 2021 to March 2022, we received a total of 2333 referrals. 81% of patients went through the novel pathway, 7% requires face-to-face appointments, 8% were referred back to GP, 2% downgraded and only 2% DNA.
In this first year, 4.4% of all referrals result in an UGI/HPB cancer diagnosis and there were additional 23 extra gastroenterology diagnosis made (0.98%). This is compatible with national 2WW outcomes. In the remainder of patients without a cancer diagnosis, 20% of all referrals had a benign condition which required follow-up and the rest were discharged back to GP.
Prior to the implementation of this pathway, we would have needed 1190 target gastroenterology clinic appointments but during this year, only 162 were required with the rest of clinics being telephone clinic with a CNS. The savings of outpatient appointments were utilised to improve routine waiting times to see a consultant.
This pathway has also reduced the number of clinic DNAs and led to improvement in our meeting the national targets. Prior to this pathway, we were meeting the FDS in 40-45% of the time. This has improved to 68-75%.
What were the learning points?
We learnt that a nurse-run digital cancer pathway is safe and allows us to improve compliance with the FDS targets. It requires engagement across multiple disciplines including IT and management. This pathway is also ever evolving as we learn from experience. Following a case of a patient referred to the cancer pathway with jaundice from auto-immune hepatitis, we have tweaked the algorithm to allow for discussion with hepatology in cases of acute transaminitis, before going straight to imaging. While this pathway is standardised, it still allows for personalisation of patient care as a consultant reviews the results of all the tests prior to discharge. When patients with benign disease are discharged off the pathway, our digital tools allows for patient information and advice to be given.
This pathway also improves our routine targets through increased utilisation of consultant clinics for routine and follow-up appointments. Following on from the success of this service, we are working towards a nurse-led IPMN surveillance pathway and also transnasal endoscopy service based in outpatients to increase our endoscopy capacity which is one limiting factor in meeting the FDS at present.