Authors:
Zameer Mohamed, Michael Carbonell, Sonia Bouri, Richard Appleby, Emma Johnston
Department of Gastroenterology, West Middlesex University Hospital, Chelsea and Westminster Hospital NHS Foundation Trust, London, UK.
What were the challenges to your service and why did you need to change?
The 2019/2020 IBD Standards highlighted four core areas for change including increased access to specialist treatment and assessment. The role of IBD clinical nurse specialists (CNS) to deliver a high quality IBD service was deemed essential. The existing IBD CNS staffing level at our unit fell well below the desired quota recommended by the IBD benchmarking framework to adequately serve the local IBD population (0.8 whole time equivalent IBD CNS vs 2.8 recommended). It was notable that from the IBD Standards patient survey for our site that patients waited longer for a response when contacting the IBD advice line and for a treatment intervention when compared to the National average. Despite increasing demands, no further funding was available at the time to increase the IBD CNS levels due to resource constraints. However, increasing resources were being made available to diversify the use of the virtual ward (VW) for all medical specialities.
The findings of an IBD VW pilot in 2022 for the management of severe Ulcerative Colitis (UC) at our site demonstrated a range of benefits including supported early discharge from hospital, low readmission rates and appropriate treatment escalation including colectomy (full results published as an abstract at BSG 2023). Although these findings were promising, it remained important to demonstrate that this model of care was sustainable and also had the potential to expand to include support for other important cohorts of patients with IBD.
How did you overcome these challenges?
A working group with all the key stake holders, including wider members of the IBD MDT (e.g. obstetrics team), was established to build on the protocol for severe UC to include pathways for Crohn’s Disease (CD), patients bridging to surgery and pregnancy (see Figure 1). Support was given from the North West London Virtual Hospital to ensure adequate capacity up upscale the IBD VW.
All patients upload their relevant clinical score daily and the VW teams were given training to conduct a telephone assessment three times a week, with pre-established escalation thresholds set. Furthermore, all patients are discussed weekly as part of the IBD MDT.
What were the outcomes?
There were 69 admissions to the VW between June 2022 and December 2023. 33 VW admissions (47.8%) were direct from inpatient admission, 8 (11.6%) from clinic, 6 (8.7%) from emergency care, and 22 (31.9%) from other sources (IBD helpline, MDT or endoscopy). The median inpatient length of stay prior to VW admission was 5.5 days (IQR 4–11). 47 (79.7%) of VW patients had UC, 22 (20.3%) had CD. 3 (4.3%) admissions were pregnant women, and 3 (4.3%) patients were specifically admitted to the VW as a bridge to surgery.
55 (79.7%) patients were on oral steroids at admission, 29 (42%) were on biologic therapy. The median length of stay on the VW was 21 days (IQR 14-28). The median SCCAI on admission was 6 (IQR 3-10), falling to 2 (IQR 1-4) on discharge. The median HBI on admission was 5 (IQR 2.5–6.25), falling to 2 (IQR 0.75–5.25) on discharge. 22 (31.9%) admissions resulted in escalation to or change in biologic therapy, with a median 10 days (IQR 3–22) to escalation. 7 (10.1%) admissions resulted in surgery, with a median 17 days (IQR 16–20) to surgery. 3 (4.3%) patients were admitted to hospital whilst on the VW and 5 (7.2%) patients had an emergency care encounter whilst on the VW that did not lead to admission.
What were the learning points and how can this influence other teams?
The IBD VW is now a well-established part of our service. It has even allowed us to manage complex and pregnant IBD patients safely and effectively as non-inpatients. Expanding the IBD CNS quota to meet the IBD benchmark standard was a fundamental issue in our unit and mirrors the challenge faced by the majority of IBD services nationally. We recognised that overburdening of our IBD CNS was likely having a negative impact on the care delivered to our IBD cohort, especially in the outpatient setting. We took advantage of the expansion of VW services within our Integrated Care System as part of an initiative to support early discharge and prevent admission. Engagement with all key stakeholders and the formation of a working group was key to successfully supporting the increased use of the IBD VW severe UC pathway and creation of other more bespoke IBD care pathways. Furthermore, the use of the IBD VW is likely to improve the efficiency within an IBD service through reallocation of IBD CNS time to focus on other essential activities.
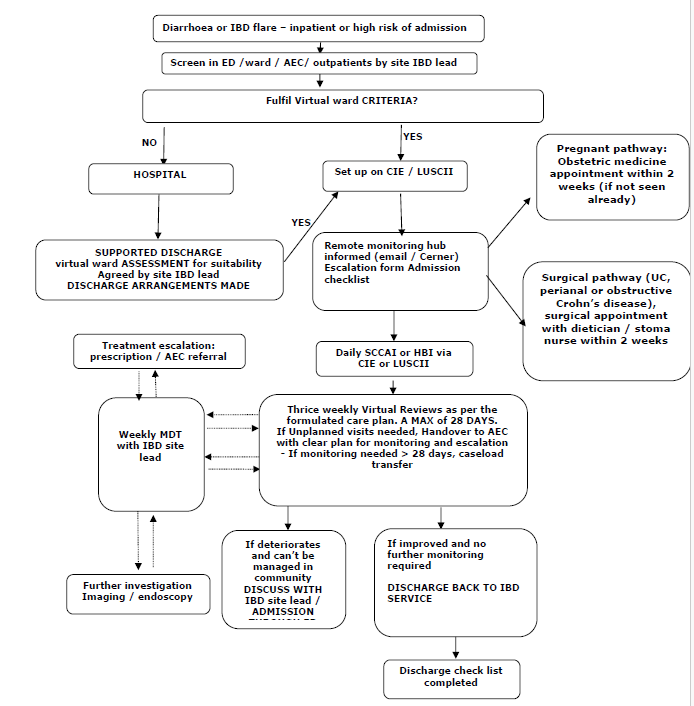
Figure 1. IBD Virtual ward pathway